REVIEW ARTICLE
Abstract
Lung cancer is a major global health problem, as it is the leading cause of cancer-related deaths worldwide. Major advances in the identification of key mutational alterations have led to the development of molecularly targeted therapies, whose efficacy has been limited by emergence of resistance mechanisms. US Food and Drug Administration (FDA)-approved therapies targeting angiogenesis and more recently immune checkpoints have reinvigorated enthusiasm in elucidating the prognostic and pathophysiological roles of the tumour microenvironment in lung cancer.
In this Review, we highlight recent advances and emerging concepts for how the tumour-reprogrammed lung microenvironment promotes both primary lung tumours and lung metastasis from extrapulmonary neoplasms by contributing to inflammation, angiogenesis, immune modulation and response to therapies.
We also discuss the potential of understanding tumour microenvironmental processes to identify biomarkers of clinical utility and to develop novel targeted therapies against lung cancer.
Introduction
Lung cancer is the leading cause of cancer-related mortality, with non-small-cell lung cancer (NSCLC) as the most prevalent form with a poor 5-year survival of ~15%1.
Despite advances in treatment options including surgery, radiation, chemotherapy and targeted therapies, prognosis remains poor owing to the presence of locally advanced or widely metastatic tumours in the majority of patients at the time of diagnosis2.
However, extensive genomic characterization of NSCLC has led to the identification of molecular subtypes of NSCLC that are oncogene addicted and exquisitely sensitive to targeted therapies3. These include activating mutations in epidermal growth factor receptor (EGFR) and BRAF or echinoderm microtubule-associated protein-like 4 (EML4)–anaplastic lymphoma kinase (ALK) fusions and ROS1 receptor tyrosine kinase fusions.
Drugs that target the tyrosine kinase domain of these driver oncogenes have resulted in improved response rates and survival in patients with metastatic disease4.
Unfortunately, this represents only 15–20% of patients and, while these interventions are effective initially, efficacy in the majority of the patients is limited by emergence of resistance mechanisms4.
Therefore, further molecular characterization of the tumour landscape has the potential to identify novel biomarkers and molecular targets that impact disease progression and enable the design of novel therapeutic strategies5.
In the past decade, the central role of the tumour microenvironment (TME) in the initiation and progression of primary de novo lung carcinoma has been recognized3,6,7.
In addition, extrathoracic malignancies including breast and colon cancer and melanoma systemically reprogramme the lung microenvironment to support the colonization and outgrowth of disseminated tumour cells (DTCs) to generate secondary lung tumours8.
The TME in both primary and secondary lung tumours is recognized as a target-rich environment for the development of novel anticancer agents. In fact, drugs targeting various components of the TME including vascular endothelial growth factor (VEGF), aromatase and immune checkpoints have already been approved for use in the clinic2.
In this Review, we summarize recent advances showing how the specialized lung TME supports both primary lung cancer and metastasis from extrapulmonary carcinoma and discuss how the mechanistic understanding of aberrant molecular signalling networks stimulated by tumour–stromal interactions has the potential to provide novel diagnostic, prognostic and therapeutic opportunities. We also highlight technological advances in live imaging, multiscale profiling and deconvolution of bulk gene expression data for mapping the microenvironmental landscape.
The altered TME landscape
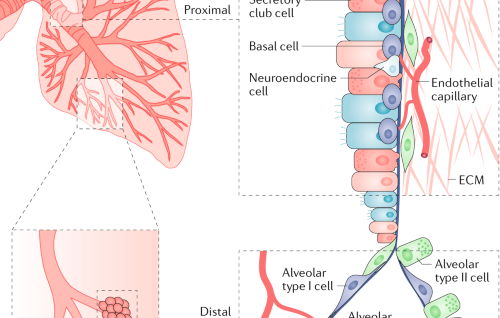
The anatomical and cellular features of the normal lung serve as a defensive barrier against foreign pathogens and particulates. However, in inflammatory states such as chronic obstructive pulmonary disease (COPD)9, the lung microenvironment displays features that may support carcinogenesis (Fig. 1).
Human lung adenocarcinomas encompass unique lung cancer subtypes with distinct cellular and mutational heterogeneity3. Importantly, this heterogeneity is not only limited to tumour epithelial cells but also spans the TME, which includes vasculature, cancer-associated fibroblasts (CAFs), extracellular matrix (ECM) and infiltrating immune cells.
In human NSCLC, stage-dependent immune cell infiltration10,11 suggests that the TME contributes to lung carcinogenesis and may have prognostic utility. As such, specific TME states are being considered as potential biomarkers to determine the stage and/or type of disease, clinical outcome and therapeutic responses (Box 1).

A schematic of the normal lung showing anatomic regions encompassing the proximal and distal airways is shown. The proximal airways are composed of ciliated cells, secretory club cells, undifferentiated basal cells, mucus-producing goblet cells and neuroendocrine cells; the distal airways are composed of alveolar type I and type II cells256. Other cell types in the lung microenvironment include smooth muscle cells, fibroblasts, endothelial cells and immune cells, including resident alveolar macrophages and dendritic cells. Vascular capillaries line the alveolar walls to facilitate gaseous exchange and infiltration of circulating immune cells257. Endothelium-derived angiocrine signalling induces and sustains regenerative lung alveolarization258,259. Resident alveolar macrophages maintain immunological homeostasis; however, they can also contribute to inflammation and the development of pre-malignant lung lesions in mice260. Patients with chronic obstructive pulmonary disease (COPD) are at a higher risk of developing lung cancer9, and their lungs show remodelling of the airway epithelium and alterations in lung inflammatory cells including neutrophils, monocytes and macrophages, which express elevated levels of pro-inflammatory mediators. A population of tissue-resident memory T cells resides in the lung airways, and they are generated by a diverse set of pathogens penetrating mucosal barriers and are believed to confer protective immunity to secondary infections261. ECM, extracellular matrix.
In the lung TME, malignant cancer cells can reprogramme the tumour-infiltrating stromal cells, which in turn contribute to carcinogenesis6,7. A growing appreciation of the role of the TME in promoting lung carcinogenesis has driven the development of anticancer therapies that target the TME. Therefore, understanding the heterotypic reciprocal crosstalk between cancer cells, various stromal cells and ECM described below is an area of active research (Fig. 2).

The lung tumour microenvironment (TME) includes a variety of tumour-reprogrammed stromal cells. A major hallmark of immunosuppression in the TME is the inactivation of cytotoxic CD8+ T cells, which is achieved through diverse pathways. Immature dendritic cells (DCs) produce transforming growth factor-β (TGFβ), which expands the population of immunosuppressive forkhead box P3 (FOXP3)+ regulatory T (Treg) cells, which in turn inhibit CD8+ T cells. DCs also express programmed cell death protein 1 (PD1) ligand 1 (PDL1) to directly suppress CD8+ T cells. Myeloid-derived suppressor cells (MDSCs) express arginase 1 (ARG1) and inducible nitric oxide synthase (iNOS), which contribute to T cell inhibition. Cancer-associated fibroblasts (CAFs) can also suppress the activity of CD8+ T cells by inducing Treg cells or by expressing PDL1, PDL2 and FAS ligand (FASL). Furthermore, tumour cells can directly produce inhibitory molecules including cyclooxygenase 2 (COX2), prostaglandin E2 (PGE2), PDL1 and indoleamine 2,3-dioxygenase (IDO), which can blunt the activity of CD8+ tumour-infiltrating lymphocytes. Neutrophils are major players in the lung TME, as they impact tumour progression through secretion of cytokines (interleukin-1β (IL-1β) and IL-6). Tumours secrete soluble receptor for advanced glycosylation end product (sRAGE), which systemically activates osteoblasts in the bone marrow to produce tumour-infiltrating sialic acid-binding immunoglobulin-like lectin F (SiglecF) neutrophils, which promote tumour growth by increasing angiogenesis, myeloid cell differentiation, T cell suppression and tumour cell proliferation. Endothelial cells respond to vascular endothelial growth factor (VEGF) from various sources including tumour cells, natural killer (NK) cells and tumour-associated macrophages (TAMs) to induce angiogenesis. In addition to promoting angiogenesis, TAMs may also activate other pathways to promote invasion and metastasis through secretion of various factors including IL-6, COX2, matrix metalloproteinase 9 (MMP9) and MMP14. Besides inducing angiogenesis, NK cells also mediate immune suppression by undergoing dysfunctional phenotypes characterized by downregulation of NK receptors, loss of degranulation potential and reduced interferon-γ (IFNγ) expression. B cells in tertiary lymphoid structures (TLS) can either generate tumour-specific antibodies or undergo a dysfunctional state that induces Treg cells. BTLA, B and T lymphocyte attenuator; CSCs, cancer stem cells; CTLA4, cytotoxic T lymphocyte-associated antigen 4; EMT, epithelial-to-mesenchymal transition; FGF4, fibroblast growth factor 4; GAS6, growth arrest-specific protein 6; HGF, hepatocyte growth factor; IGF1R, insulin-like growth factor 1 receptor; IGF2, insulin-like growth factor 2; LAG3, lymphocyte activation gene 3; PDGFβ, platelet-derived growth factor-β; PlGF, placental growth factor; STAT, signal transducer and activator of transcription; TIM3, T cell membrane protein 3; TNF, tumour necrosis factor.
Cancer-associated fibroblasts
Human NSCLC often exhibits desmoplasia, which is characterized by the presence of CAFs12.
In solid tumours, CAFs mediate cancer cell proliferation, angiogenesis, invasion, metastasis and drug resistance13.
CAFs isolated from human lung cancer tissues secrete interleukin-6 (IL-6), which stimulates Janus kinase 2 (JAK2)–signal transducer and activator of transcription 3 (STAT3) signalling in human lung cancer cells to increase metastasis in vivo14.
CAFs also express insulin-like growth factor 2 (IGF2), which through ligation of the IGF1 receptor (IGF1R) on cancer stem cells (CSCs) induces expression of the stemness marker NANOG, leading to CSC enrichment15.
CAFs also drive expression of α11β1 integrin, leading to increased ECM stiffness that contributes to increased growth and metastasis of patient-derived xenografts16,17.
Intriguingly, one study showed that CAFs from human NSCLC exhibit increased autophagy and glycolytic metabolism18; however, the consequences of this finding in carcinogenesis remain unknown.
CAFs also modulate immune responses in the TME. For example, CAFs isolated from a subset of human NSCLC expressing the ligands of the programmed cell death protein 1 (PD1) receptor, PD1 ligand 1 (PDL1) and PDL2, were shown to suppress T cell function in coculture experiments19.
Similarly, in a genetic mouse model of lung cancer, CAFs were able to cross-present antigens complexed with major histocompatibility complex class I (MHC I) to antigen-specific CD8+ T cells, leading to antigen-specific upregulation of PDL2 and FAS ligand (FASL) within these T cells and resulting in their elimination20.
The response to chemotherapy can also be modulated by CAFs, as cisplatin-induced expression of the receptor tyrosine kinase AXL (also known as UFO) ligand growth arrest-specific protein 6 (GAS6) in CAFs promoted migration of AXL-expressing lung cancer cells in mice21.
Consistent with these findings in mice, the 5-year disease-free survival was significantly worse in patients with AXL+ tumour cells and GAS6+ stroma, suggesting the potential of combining chemotherapy with AXL or GAS6 inhibition22.
Given the multifaceted nature of CAFs, it will be important for future studies to identify factors that drive the transcriptional reprogramming of CAFs in the lung TME, as this may aid the development of CAF-targeting therapies.
Extracellular matrix
The ECM, composed of collagens, proteoglycans and glycosaminoglycans, is a major constituent of the TME and mediates interactions between cancer cells and stromal cells to promote carcinogenesis23. In the KRAS-driven NSCLC mouse model (KrasG12D;Trp53fl/fl), matrix metalloproteinase 14 (MMP14) expressed on the membranes of both cancer cells and myeloid cells mediated proteolytic processing of heparin-binding EGF-like growth factor (HB-EGF), leading to its activation; activated EGF stimulated the EGFR signalling pathway to promote tumour growth24. In another study, the receptor for the glycosaminoglycan hyaluronan, known as hyaluronan-mediated motility receptor (HMMR), enhanced ECM-mediated signalling and promoted tumour outgrowth in the lung following intratracheal administration of human tumour cells in mice25. Loss-of-function mutations in the tumour suppressor LKB1 (also known as STK11), which are observed in ~30% of KRAS-mutated human lung adenocarcinomas, contribute to multiple cellular functions including cellular metabolism, cell polarity, invasion and metastasis26. In mice, LKB1 deficiency upregulated the ECM protein lysyl oxidase through the mTOR–hypoxia-inducible factor 1α (HIF1α) signalling axis, which in turn mediated collagen crosslinking and β1 integrin signalling activation27. Together, these studies suggest that targeting the ECM network including MMP14, hyaluronan and lysyl oxidase has potential therapeutic value. ECM density has also been shown to function as a major barrier to T cell infiltration into tumour beds in human NSCLC28. Therefore, targeting the ECM network may facilitate T cell infiltration into tumour beds for effective antitumour efficacy.
Endothelial cells
Angiogenesis, the formation of new blood vessels from pre-existing vasculature, is a key hallmark of cancers29. Tumour-derived angiogenic factors contribute to endothelial cell migration and proliferation, leading to formation of new blood capillaries that support tumour progression, invasion and metastasis. Several angiogenesis inhibitors including bevacizumab have either been approved or are in clinical trials for the treatment of NSCLC; however, it is striking that mechanistic insights into angiogenesis in lung carcinogenesis are limited. In the KRAS-driven mouse model, endothelial expression of the microRNAs (miRNAs) miR-143 and miR-145 promoted angiogenesis-mediated tumour growth30, suggesting the therapeutic potential of endothelial-specific inhibition of these miRNAs. The NAD-dependent protein deacetylase sirtuin 1, a key regulator of angiogenesis, was shown to increase vessel density and promote the growth of Lewis lung carcinoma (LLC) xenografts by downregulating delta-like ligand 4 (DLL4)–Notch signalling and through deacetylation of the NOTCH1 intracellular domain in lung cancer-derived endothelial cells31.
However, the prevailing concept that tumour growth is strictly dependent on neo-angiogenesis has been challenged, as a subset of patients with NSCLC exhibit non-angiogenic growth patterns. These tumours appear to exploit pre-existing blood vessels rather than induce angiogenesis and importantly have a worse prognosis than their angiogenic counterparts32. Hence, it is unlikely that antiangiogenic treatments would be effective for all patients with lung cancer, and this may explain the modest clinical benefits associated with antiangiogenic therapies in NSCLC. Therefore, understanding the complex biology of the tumour vasculature and angiogenic signalling in NSCLC constitutes an important area of research. Indeed, analysis of 180 human NSCLC specimens captured multiple unique and dominant angiogenic phenotypes33. Given that angiogenesis is dependent on a complex network of different cellular compartments regulated by a balance of angiogenic and antiangiogenic factors, a greater understanding of tumour-specific angiogenesis has the potential to aid the rational design of antiangiogenic interventions.
The immune TME
The innate and adaptive immune cells in the lung TME harbour both tumour-promoting and tumour-suppressing activities, which may also predict clinical outcome34,35. Genome-wide expression analysis has begun to provide molecular insights into the tumour-induced reprogramming of infiltrating lymphoid and myeloid cells in both mouse and human NSCLC36,37.
Myeloid cell populations
Myeloid cells of granulocytic and monocytic lineages are components of innate immunity and contribute to carcinogenesis in various ways38,39. Myeloid cells can also regulate adaptive immunity by controlling tumour-infiltrating lymphocyte (TIL) composition, activation and antitumour function40. Major efforts in the field are now directed towards developing a comprehensive atlas of the immune TME. Indeed, recent analysis of myeloid cells from tumours and matched adjacent non-neoplastic lung tissue of patients with NSCLC identified differentially regulated genes36,37, and a comprehensive analysis in the KRAS-driven mouse model unravelled myeloid–tumour crosstalk networks41. Insights from such analyses have the potential to enable the design of therapeutic strategies that target tumour–stroma crosstalk pathways.
Dendritic cells (DCs) are myeloid derived and recognized as central orchestrators of antitumoural immunity by virtue of their ability to cross-present tumour antigens to prime T lymphocytes in the draining lymph nodes42. However, tumours can suppress DC function or alter the TME to recruit immune-suppressive DCs. In patients with NSCLC, DCs upregulate the co-inhibitory molecule B7-H3 (also known as CD276) and therefore fail to stimulate T cells43. Human DCs also produce transforming growth factor-β (TGFβ), which induces the differentiation of CD4+ T cells into CD4+CD25+forkhead box P3 (FOXP3)+ regulatory T (Treg) cells that suppress T cell proliferation44. A preclinical study showed that administration of DCs transduced with the chemoattractant CC-chemokine ligand 21 (CCL21) led to increased infiltration of DCs and CD4+ and CD8+ T cells in the lung TME, resulting in reduced tumour burden45. These findings led to a phase I trial being conducted in patients with advanced NSCLC in which intratumoural vaccination with autologous DCs expressing CCL21 showed an increase in CD8+ T cell infiltration into tumours, as well as increased PDL1 expression on tumour cells46. Given that the efficacy of DC vaccines as a monotherapy is limited by immunosuppressive mechanisms in the TME, these results provide a rationale for combining immunotherapy with in situ vaccination. More recently, DC vaccine platforms have begun to incorporate innovative approaches for improving DC maturation, proliferation, antigen presentation and selection and have been used in combination with other therapies including immune checkpoint inhibitors and standard of care therapies in solid tumours including NSCLC47.
Myeloid-derived suppressor cells (MDSCs) are a heterogeneous cell population that can suppress T cell proliferation and cytokine production38. Currently, MDSCs can be further divided into two major subsets: polymorphonuclear MDSCs (PMN-MDSCs) and monocytic MDSCs (M-MDSCs). PMN-MDSCs share many morphological and phenotypic characteristics of neutrophils, whereas M-MDSCs are more similar to immature monocytes. However, they also have different molecular and biochemical characteristics, which have not been completely characterized48,49. In both mice and human cancers, PMN-MDSCs that phenotypically resemble neutrophils represent the most abundant population of MDSCs49. A study in patients with NSCLC showed that endoplasmic reticulum stress-driven inositol-requiring protein 1 (IRE1; also known as ERN1)–X-box binding protein 1 (XBP1) signalling converts regular neutrophils into highly immunosuppressive lectin-type oxidized low-density lipoprotein receptor 1 (LOX1)+ PMN-MDSCs50. Given the marked increase of LOX1+ MDSCs in patients with NSCLC, future studies are likely to assess the potential of LOX1+ cells as a prognostic biomarker in NSCLC treatment. Additionally, either eliminating LOX1+ PNM-MDSCs or targeting the IRE1–XBP1 pathway that contributes to the generation of these cells may have potential therapeutic application in NSCLC.
Tumour-associated macrophages (TAMs) are abundant components of the NSCLC immune infiltrate51, are highly plastic and display a variety of phenotypes, including M1 (classically activated, pro-inflammatory with antitumour activity) and M2 (alternatively activated, proangiogenic and immunosuppressive with protumour activity), which are governed by the nature of the local microenvironments51,52. The current view is that the different macrophage phenotypes present within the TME is a continuum and therefore cannot be captured solely with the M1–M2 dichotomy53. Given this heterogeneity of phenotypes, the prognostic relevance of TAMs in NSCLC remains unresolved54, and future studies aimed towards a more comprehensive analysis of the clinical importance of TAMs in NSCLC are needed. In the KRAS-driven mouse model, TAMs expressing IL-6 interact with IL-6 receptors on cancer cells, leading to the activation of tumour-promoting STAT3 signalling41. Lungs also harbour resident alveolar macrophages, which promote carcinogenesis in mice55,56. While macrophage depletion impacts tumour growth in a carcinogen-induced model of lung adenocarcinoma56, TAM targeting with inhibitors of colony-stimulating factor 1 receptor (CSF1R) have exhibited limited benefit in clinical trials57. In one preclinical study, as expected, CSF1R inhibition effectively eliminated TAMs; however, an unexpected accumulation of immunosuppressive PMN-MDSCs triggered by CXC-chemokine ligand 1 (CXCL1) released from CAFs was observed58. Notably, combined inhibition of CSF1R and CXC-chemokine receptor 2 (CXCR2) (the receptor for CXCL1) decreased PMN-MDSC recruitment and abrogated tumour growth58. The existence of this mechanism in human NSCLC has not been investigated.
Neutrophils infiltrating mouse tumours can either promote carcinogenesis by supporting tumour-related inflammation, angiogenesis and metastasis or restrict tumour growth through the expression of antitumour and cytotoxic mediators59,60. However, such functional diversity has not been evaluated in human lung cancer. In human NSCLC, neutrophils dominate the immune landscape11. A recent study identified a unique subset of tumour-infiltrating neutrophils that expressed markers of both neutrophils and antigen-presenting cells (APCs), enabling this cell type to cross-present antigens, as well as augment antitumour T cell responses61. Neutrophils also express IL-1β, which mediates resistance to nuclear factor-κB (NF-κB) inhibitors in the KRAS-driven mouse model62. Furthermore, neutrophil depletion was associated with a pronounced reduction in lung carcinogenesis in LLC xenograft and carcinogen (methylcholanthrene)-induced mouse models of lung cancer37,63. A recent study showed that secretion of soluble receptor for advanced glycosylation end product (sRAGE) by KRAS-driven lung adenocarcinomas systemically activated osteocalcin-positive osteoblasts in the bone marrow of mice64. Bone marrow activation led to the production of sialic acid-binding immunoglobulin-like lectin F (SiglecF; also known as Siglec5) neutrophils that homed to the lungs to promote tumour growth by promoting angiogenesis, myeloid cell differentiation, T cell suppression and tumour cell proliferation. While the relevance of this type of neutrophils in humans remains unknown, the authors did identify a SiglecFhigh neutrophil signature that was associated with poor patient survival in patients with lung cancer. Future studies characterizing tumour-infiltrating neutrophil phenotypes during human NSCLC progression may allow precise targeting to eliminate specific pro-tumorigenic subsets or increase the activity of antitumorigenic subsets.
Natural killer (NK) cells are lymphocytes of the innate immune system that play a key role in antitumour immunity by virtue of directly recognizing tumour cells as targets65. As cancer cells have evolved multiple strategies to escape CD8+ T cell recognition, the importance of NK cells in directly mediating tumour cell destruction has recently gained prominence66. Several studies have characterized the frequency, localization, phenotype and functional status of NK cells infiltrating the lung TME in mice and humans67. Factors that regulate NK cell response in the lung TME include TGFβ, which mediates polarization of NK cells towards a proangiogenic phenotype, as determined by expression of VEGF, placental growth factor (PlGF) and interferon-γ (IFNγ)68. A dysfunctional state of NK cells was associated with downregulation of NK cell receptors, decreased degranulation and loss of IFNγ expression in human NSCLC67. Despite these findings, NK cells from pleural effusions of patients with lung cancer expressed MHC I and released cytokines upon exposure to both allogeneic and autologous tumour cells in vitro69. While insights into NK cell biology have increased in recent years, NK cell subset identification and function in lung carcinogenesis remain to be elucidated.
Lymphoid cell populations
T lymphocytes infiltrating tumours, particularly the CD4+ and CD8+ T cells, and their immunoregulatory cytokines represent adaptive immunity, execute key effector cytotoxic functions in the TME and mediate responses to immune checkpoint inhibition (ICI). In the KRAS-driven mouse model, PD1 inhibition resulted in increased proliferation of all T cell subsets and effector cytokine production by CD4+ T helper 1 (TH1) cells, while the depletion of CD4+ and/or CD8+ T cells in combination with a PD1 antibody resulted in reduced therapeutic efficacy of the PD1 blockade70.
Immunosuppressive FOXP3+ Treg cells are induced by cyclooxygenase 2 (COX2; also known as PTGS2)-mediated upregulation of prostaglandin E2 (PGE2) in tumour cells71. As expected, Treg cell depletion reduced lung tumour burden in mice72 and was associated with an increased expression of granzyme A, granzyme B, perforin and IFNγ in CD8+ TILs73. In the KRAS-driven mouse model, PD1 inhibition was associated with upregulation of PD1 and IFNγ in a proportion of Treg cells, suggesting loss of immunosuppressive activity70. Within the CD4+ T cell populations, a fine balance between the immunosuppressive Treg cells and pro-inflammatory TH17 cells is associated with effective adaptive immune responses in lung carcinogenesis74. However, given the context-dependent pro-tumorigenic and antitumorigenic roles of TH17 cells, further investigations are needed to characterize the mechanistic and prognostic value of these two populations in NSCLC75,76.
CD8+ cytotoxic T cells elicit tumour clearance by targeting tumour cells for destruction through production of IFNγ, tumour necrosis factor (TNF) and granzyme B after ligation of their T cell receptors (TCRs)77. However, progressing tumours employ various means of inhibiting CD8+ T cells. For example, Treg cells can directly suppress the antitumour function of CD8+ T cells73. Furthermore, persistent antigen exposure can lead to T cell dysfunction or exhaustion characterized by loss of effector and memory functions, a phenomenon first recognized in the setting of chronic viral infections78. In patients with NSCLC, disease progression is correlated with increased expression of markers of T cell exhaustion including PD1, T cell membrane protein 3 (TIM3; also known as HAVCR2), cytotoxic T lymphocyte-associated antigen 4 (CTLA4), lymphocyte activation gene 3 (LAG3) and B and T lymphocyte attenuator (BTLA) on CD8+ TILs79. Indeed, treatment with anti-PD1 therapy increased the number of highly proliferative (Ki67+) PD1+ CD8+ T cells in the circulation of patients with NSCLC80. Despite the central role of CD8+ T cells in antitumour immunity, an efficient antitumour immune response requires the cooperation of both CD8+ and CD4+ T cells, as the therapeutic efficacy of PD1 inhibition was only partially reversed by depletion of CD8+ T cells but was completely abolished by the additional depletion of CD4+ T cells in the KRAS-driven mouse model70.
Tumour-infiltrating B cells have emerged as key players in the TME. In patients with NSCLC, tumour-infiltrating B cells and CD4+ T cells reside within the tertiary lymphoid structures (TLS), and these structures correlate with better prognosis81. It was demonstrated that tumour-infiltrating B cells harvested from patients can present endogenous tumour antigens to CD4+ TILs and alter the CD4+ TIL phenotype in vitro82. Interestingly, activated tumour-infiltrating B cells were associated with activated IFNγ+CD4+ T cells, and exhausted tumour-infiltrating B cells were associated with immunosuppressive Treg cells82. These studies suggest that in the TME, the ability of tumour-infiltrating B cells to influence CD4+ TILs constitutes a potential novel therapeutic target in NSCLC immunotherapy.
Immunosuppressive mechanisms
Improving the efficacy of immunotherapy requires a better understanding of the immunomodulatory roles of the immune cells within the TME83. Therefore, understanding cancer cell-intrinsic and cell-extrinsic pathways that influence the immune microenvironment has emerged as an active area of investigation.
In the context of cancer cell-intrinsic pathways of immunosuppression, a major effort is directed towards understanding how cancer cells have devised means to suppress the tumoricidal capabilities of the immune cells. Emerging studies have begun to show that oncogenic driver mutations in KRAS, p53 and EGFR are associated with discrete immune phenotypes in both mice and human lung adenocarcinomas84. Accordingly, there is marked interest in understanding exactly how these cancer cell-intrinsic pathways alter immune cells in the TME85, and some of these mechanisms are displayed in Fig. 3.

Lung adenocarcinomas with specific driver mutations exhibit discrete immune phenotypes. The observation that programmed cell death protein 1 (PD1) ligand 1 (PDL1) expression was increased in patients with KRAS-mutant lung cancer led to the finding that mutant KRAS in mouse tumours induces PDL1 expression either through phosphorylated ERK (pERK) signalling or Pdl1 mRNA stabilization to mediate immune escape262,263. These studies advocate the use of either ERK inhibitors or inhibition of the AU-rich element-binding protein tristetraprolin (TTP), which is responsible for PDL1 stabilization, for the treatment of KRAS tumours. Loss of the tumour suppressor LKB1 in KRAS-mutant mouse tumours is associated with increased accumulation of immunosuppressive neutrophils, exhausted T cells, increased pro-inflammatory cytokines including interleukin-6 (IL-6) and decreased PDL1 expression. While PD1 monotherapy was ineffective in this setting, its therapeutic efficacy can be restored with either neutrophil depletion or an IL-6-neutralizing antibody166. Similarly, immune suppression in KRAS-mutant mouse tumours may be a result of MYC co-activation leading to upregulation of IL-23 and CC-chemokine ligand 9 (CCL9), which mediates the exclusion of B cells, T cells and natural killer (NK) cells, as well as the recruitment of proangiogenic macrophages264. As expected, inhibition of CCL9 and IL-23 can decrease MYC-induced tumour progression. Clinical observations that epithelial growth factor receptor (EGFR)-mutant tumours are associated with high PDL1 expression265 are consistent with the observation that EGFR-driven mouse tumours suppress T cell function by activating PD1 and PDL1 (ref.266). Patients with echinoderm microtubule-associated protein-like 4 (EML4)–anaplastic lymphoma kinase (ALK) fusion oncogene-driven lung cancer also show increased PDL1 expression and, in mice, it was found that EML4–ALK-mediated activation of the PI3K–AKT and MEK–ERK pathways upregulates PDL1 expression267. In carcinogen-induced lung tumorigenesis, signal transducer and activator of transcription 3 (STAT3) activation in cancer cells inhibits pro-inflammatory chemokines, increases major histocompatibility complex class I (MHC I) expression, decreases effector cytokines and blunts NK cell-mediated toxicity268. Despite these findings, the link between oncogenic drivers and PDL1 expression remains controversial, as one study demonstrated an association of PDL1 expression with mutant EGFR but not KRAS or ALK in patients with non-small-cell lung cancer (NSCLC)269, while another study failed to correlate PDL1 expression with mutant EGFR in patients147. In yet another study, PDL1 expression was associated with mTOR activation in patients with NSCLC driven by a wide spectrum of driver mutations, and the combination of mTOR and PD1 inhibitors could reduce tumour growth, increase tumour-infiltrating lymphocytes and decrease regulatory T (Treg) cells in mouse lung cancers270. An emerging concept lends support for oncogene cooperativity in driving immune evasion. Co-activation of KRAS and MYC or PI3K and Kelch-like ECH-associated protein 1 (KEAP1)–nuclear factor erythroid-2-related factor 2 (NRF2) reprogrammes the tumour microenvironment (TME) to promote lung adenocarcinoma264,271. Indeed, genetic deficiency of Keap1 and Pten can increase the efficacy of immune checkpoint inhibition271. As cancer cell-intrinsic pathways alter immunity in unique ways, this calls for studies involving large cohorts of patients with NSCLC to establish how specific genomic alterations impact the TME composition and function; this would be valuable for designing combination treatments for patients who have been selected on the basis of their tumour genomic alterations and immune contexture. CTLA4, cytotoxic T lymphocyte-associated antigen 4; CXCL, CXC-chemokine ligand; G-CSF, granulocyte colony-stimulating factor; IFNγ, interferon-γ; NF-κB, nuclear factor-κB; TGFβ, transforming growth factor-β; TNF, tumour necrosis factor.
With respect to tumour-extrinsic mechanisms mediating immunosuppression, a major focus is to understand the contributions of the reprogrammed tumour-infiltrating immune cells. MDSCs express L-arginase and inducible nitric oxide synthase (iNOS), which deplete L-arginine in the TME; loss of L-arginine downregulates TCR expression, leading to T cell dysfunction, and confers poor survival in patients with NSCLC86,87. The tryptophan-catabolizing enzyme indoleamine 2,3-dioxygenase (IDO), which is expressed by a variety of cells including tumour cells, macrophages and DCs, has emerged as a potent mediator contributing to the immune escape of tumours, as tryptophan deficiency results in MDSC expansion, decreased cytotoxic T lymphocyte response and Treg cell accumulation. In KRAS-driven mouse models, IDO increased metastasis through IL-6-dependent inflammation and MDSC-driven immune escape88. IDO can metabolically reprogramme immune cells, as IDO deficiency in MDSCs was shown to downregulate nutrient-sensing AMP-activated protein kinase (AMPK) activity, leading to their inactivation, whereas in CD8+ T cells, IDO deficiency increased AMPK activation associated with an enhanced effector function in an LLC xenograft mouse model89. Thus, IDO inhibition may represent a two-pronged therapeutic approach for inhibiting MDSCs while simultaneously eliciting effector CD8+ T cells. Unfortunately, a recent phase III trial (ECHO-301)90 of IDO inhibition in combination with ICI failed in patients with melanoma, resulting in a major set-back for IDO-based immunotherapy regimens. As the ECHO-301 trial90 did not measure IDO expression to stratify patients, future studies will need to identify biomarkers that better predict responders to IDO-based therapy combinations.
The lung as a site of metastasis
The lung is also a frequent site of metastases formation from a variety of extrathoracic malignancies91,92. Malignancies including breast, skin and colon cancer secrete factors and extracellular vesicles, which systemically reprogramme the lung microenvironment to generate pre-metastatic niches. Studies in mouse models have shown that these pre-metastatic niches, which are characterized by host immune and inflammatory cells, organ-specific chemoattractants, growth factors and ECM-modifying proteins, provide permissive microenvironments that support extravasation, colonization and metastatic outgrowth of DTCs8,93 (Fig. 4).

Primary tumours secrete various growth factors, cytokines and enzymes (vascular endothelial growth factor A (VEGFA), placental growth factor (PlGF), transforming growth factor-β (TGFβ), tumour necrosis factor (TNF) and lysyl oxidase) and shed extracellular vesicles into the circulation that systemically impact the lung microenvironment. Tumour-derived factors can also activate bone marrow compartments, resulting in the mobilization and recruitment of bone marrow-derived cells into the lungs. Together, these activities contribute to the generation of pre-metastatic niches in the lung. Extravasation of disseminated tumour cells (DTCs) into the lung parenchyma is facilitated by microRNA miR-105 delivered by breast cancer exosomes, which silence the tight junction protein zona occludens 1 (ZO1) to allow DTCs to breach vascular barriers. In addition, CC-chemokine ligand 2 (CCL2) gradients recruit CC-chemokine receptor 2 (CCR2)+ inflammatory monocytes, which produce VEGF to increase vascular permeability. Following extravasation, the pre-metastatic niche contributes to the seeding and colonization of the DTCs in the lungs. Hypoxia in primary breast tumours upregulates lysyl oxidase, which systemically oxidizes lysine residues in collagen and elastin, resulting in covalent crosslinking of these molecules in the lungs. Collagen crosslinking increases the adhesion of myeloid cells to generate microenvironments conducive to DTC colonization. Platelets secrete CXC-chemokine ligand 5 (CXCL5) and CXCL7, which recruit granulocytes to facilitate metastatic seeding170. Exosome-derived small nuclear RNAs (snRNAs) activate Toll-like receptor 3 (TLR3) in lung alveolar type II cells to induce chemokine secretion, which in turn mediates neutrophil recruitment. Neutrophils, via arachidonate 5-lipoxygenase (ALOX5)-dependent leukotriene synthesis, stimulate adhesion, chemotaxis and vascular permeability to support colonization of leukotriene receptor-positive DTCs. In addition, the extracellular matrix (ECM) component fibronectin enables clustering of bone marrow-derived VEGF receptor 1 (VEGFR1)+ haematopoietic cells, leading to increased production of CXCL12, which recruits CXC-chemokine receptor 4 (CXCR4)+ DTCs to the pre-metastatic niche272. Following seeding of DTCs, α4 integrin-expressing macrophages interact with vascular cell adhesion protein 1 (VCAM1)+ DTCs to induce pro-survival AKT signalling. The polarized neutrophils in the pre-metastatic lungs may suppress activation of CD8+ T cells to dampen anti-metastatic immunity. Subsequently, metastatic outgrowth is supported by various pathways. Neutrophils may secrete cathepsin G and neutrophil elastase to proteolytically degrade the antitumorigenic factor thrombospondin 1 (TSP1) to promote the metastatic outgrowth. Tumour-secreted factors induce expression of chemoattractants, such as S100A8 and S100A9, by lung endothelial cells and MAC1 (also known as CD11b)+ myeloid cells, which facilitate the homing of tumour cells to the pre-metastatic niche, through the induction of serum amyloid A3 (SAA3)273. Notably, SAA3 stimulates nuclear factor-κB (NF-κB) signalling in a TLR4-dependent manner to facilitate inflammation-mediated metastasis. DTCs can induce expression of periostin or tenacin C in lung fibroblasts to support cancer stem cell (CSC) maintenance and expansion through WNT and Notch signalling, respectively. The colonized mesenchymal tumour cells may undergo an epithelial conversion that is supported by paracrine interactions with reprogrammed monocytic cells. The myeloid-derived proteoglycan versican mediates inhibition of the TGFβ–SMAD2 or SMAD3 pathway in DTCs that induces mesenchymal-to-epithelial transition (MET) and promotes metastatic outgrowth. Through another mechanism, mesenchymal DTCs can also express TSP2 to activate local fibroblasts, which in turn promote MET of cancer cells106. Lastly, metastatic outgrowth can be facilitated by infiltrating bone marrow-derived endothelial progenitor cells (EPCs) and endothelial cells, which contribute to the switch to angiogenesis. The pre-metastatic niche can exhibit features of metastasis suppression, as lung endothelial cells expressing CX3C-chemokine ligand 1 (CX3CL1) attract CX3C-chemokine receptor 1 (CX3CR1)+ patrolling monocytes, which through expression of CCL3, CCL4 and CCL5 recruit cytotoxic natural killer (NK) cells to inhibit metastasis. Similarly, metastatic incompetent tumours express the glycoprotein prosaposin, which systemically reprogrammes myeloid cells in the lungs to express TSP1, which inhibits metastatic outgrowth. G-CSF, granulocyte colony-stimulating factor; IL-1β, interleukin-1β; LY6C, lymphocyte antigen 6C; MMP9, matrix metalloproteinase 9.
Following dissemination into the circulation, DTCs extravasate into the lung parenchyma by breaching lung endothelial barriers94,95. Following extravasation, several mechanisms within the pre-metastatic niche facilitate DTC colonization. Hypoxia in the primary breast tumour induced by elevated levels of HIF1α triggers expression of lysyl oxidases, which systemically crosslinks collagen in the lungs, increasing the adhesion of myeloid cells to generate niches that support colonization96. In another mechanism, lung alveolar type II cells induce chemokine secretion that recruits neutrophils97. Neutrophils, via arachidonate 5-lipoxygenase (ALOX5)-dependent leukotriene synthesis, support proliferation and colonization of leukotriene B4 receptor 2 (LTB4R2)-positive DTCs98. Polarized neutrophils in the pre-metastatic lungs can also suppress activation of CD8+ T cells to dampen anti-metastatic immunity99. Furthermore, neutrophils can secrete cathepsin G and neutrophil elastase to degrade the antitumorigenic factor thrombospondin 1 (TSP1), thereby promoting metastases in the lung100. A recent study showed that atypical chemokine receptor 2 (ACKR2) expressed on haematopoietic progenitor cells restrains myeloid differentiation and function, and targeting host ACKR2 increased the ability of neutrophils to target to lung metastases in a breast cancer mouse model101.
Following colonization, it is important for DTCs to be able to survive in the foreign microenvironment of the metastatic lung, and this is known to be facilitated by α4 integrin-expressing macrophages, which induce pro-survival AKT signalling in DTCs102. DTCs also exploit fibroblasts to produce periostin and tenascin C, which induce WNT and Notch signalling, respectively, in DTCs to promote expansion103,104. Mesenchymal tumour cells may undergo an epithelial conversion (mesenchymal-to-epithelial transition (MET)), which is supported by the myeloid-derived proteoglycan versican105 or through activated, local fibroblasts generated by tumour-derived TSP2 (ref.106). In addition, metastatic outgrowth is supported by angiogenesis, which is mediated by infiltrating bone marrow-derived endothelial progenitor cells107 or VEGF-induced VEGF receptor 2 (VEGFR2) phosphorylation that in turn triggers calcineurin–nuclear factor of activated T cells (NFAT) signalling to transactivate the angiogenic growth factor angiopoietin 2 (ANG2) in the lung endothelium108.
NK cells have been recognized to play an important role in tumour immunosurveillance and metastasis control109. The discovery that CD96 is a negative regulator of NK cell activity led to the use of CD96-neutralizing antibodies in preclinical models. These antibodies enhanced NK cell IFNγ-dependent effector function to inhibit lung metastasis in mice110,111. However, in the context of the pre-metastatic niche, hypoxic tumour cell-derived CCL2, by virtue of recruiting granulocytic myeloid cells from the bone marrow to the lungs, creates an immunosuppressive pre-metastatic niche through suppression of NK cell cytotoxicity and maturity112. Importantly, a recent study identified an NK cell checkpoint IL-1 receptor 8 (IL-1R8; also known as SIGIRR), which restrains NK cell maturation and effector function; inhibition of IL-1R8 unleashed NK cells to impair metastasis in the lungs of mice113.
Intriguingly, some studies have also described metastasis-suppressive niches. For instance, certain metastatic incompetent tumours express the glycoprotein prosaposin, which systemically reprogrammes myeloid cells in the lungs to express TSP1, generating metastasis-suppressive niches in mice114. Similarly, lung endothelial cells expressing CX3-chemokine ligand 1 (CX3CL1; also known as fractalkine) attract -CX3C-chemokine receptor 1 (CX3CR1)+ patrolling monocytes, which through expression of CCL3, CCL4 and CCL5 recruit cytotoxic NK cells to prevent metastasis to the lung in mice115.
Local pre-existing inflammation in the lung caused by exposure to cigarette smoke may contribute to increased metastasis. For example, cigarette smoke-induced inflammation is correlated with increased metastasis to the lungs from primary breast cancers in mice and humans116,117. The mechanisms governing metastasis-promoting effects of inflammation include the ubiquitin–CXCR4 signalling axis118, elevated levels of E-selectin expression in lung tissue119 and NF-κB activation in airway epithelial cells120 or increased CCL2 expression and macrophage infiltration in the lung microenvironment121. Recently, it was shown that T cell-intrinsic expression of oxygen-sensing prolyl hydroxylase domain (PHD) proteins restrained lung inflammation by decreasing TH1 cell differentiation, inducing Treg cells and suppressing CD8+ T cell effector function122. DTCs can exploit these immunologically tolerant metastatic niches for metastatic progression122.
In many patients, DTCs that colonize the lungs may undergo dormancy, and targeting dormancy constitutes an attractive therapeutic strategy for minimizing the risk of cancer recurrence123,124. While mechanisms underlying cancer cell-intrinsic pathways of dormancy regulation are beginning to be identified123,124, emerging evidence also implicates the contribution of the local microenvironment125,126 (Box 2). Primary lung adenocarcinomas also exhibit metastasis, with the common metastatic sites being the bone, brain, liver and adrenal glands. The contribution of specialized microenvironments that support colonization and progression of metastases is now being elucidated127 (Box 3).
The lung TME as a target for therapy
The identification of critical cellular and molecular pathways in the TME has yielded potential strategies to target key cancer vulnerabilities6,128 (Table 1), and drugs targeting TME components are being investigated in clinical trials (Supplementary Table 1).
Antiangiogenic therapies
The VEGF pathway is a key mediator of tumour angiogenesis, and angiogenesis inhibitors targeting various components of this pathway including VEGF ligands, VEGFRs and downstream signalling components have been developed. These agents have been extensively tested in advanced NSCLC, some of which have been approved by the US Food and Drug Administration (FDA)129. The VEGF antibody bevacizumab was FDA-approved in 2006 for use in combination with carboplatin and paclitaxel chemotherapy as a first-line treatment for advanced, non-squamous NSCLC130. Additionally, ramucirumab, a VEGFR2-targeting antibody, has been approved in combination with docetaxel chemotherapy for the treatment of patients with metastatic NSCLC who have progressed on or after platinum-based chemotherapy131. Finally, nintedanib, an antibody targeting the tyrosine kinases VEGFR1, VEGFR2, VEGFR3, platelet-derived growth factor receptor-α (PDGFRα), PDGFRβ, fibroblast growth factor receptor 1 (FGFR1), FGFR2 and FGFR3, has been approved by the European Union for use in combination with docetaxel for the treatment of patients with advanced NSCLC with disease progression after front-line platinum-based chemotherapy132. Currently, a plethora of antiangiogenic agents including aflibercept (known as a ‘VEGF trap’, as it binds to circulating VEGF ligands) and the receptor tyrosine kinase inhibitors sunitinib, sorafenib, motesanib, cediranib and vandetanib are being evaluated in clinical trials133.
Despite documented benefits, results from phase III clinical trials have shown that treatment with antiangiogenic therapies is often associated with somewhat modest increases in median overall survival (OS) and progression free survival (PFS) (Supplementary Table 1). With a growing number of antiangiogenic agents being approved or considered for approval, the requirement for biomarkers is critical for determining drug efficacy and safety, as patient selection may be key to improving these modest clinical benefits seen to date.
Anti-inflammatory therapies
Epidemiological evidence and clinical trial results have indicated that long-term use of aspirin, which is primarily designed to prevent cardiovascular disease, is associated with a reduction in cancer deaths after long-term follow-up134,135. By contrast, a large population-based study, showed a lack of association between aspirin use before diagnosis and lung cancer-specific mortality136. A meta-analysis of several studies related to aspirin use revealed heterogeneous responses, suggesting that it may be important to identify particular patient populations that could benefit from aspirin use137. The COX2 inhibitor celecoxib initially displayed clinical benefit in patients with high COX2-expressing NSCLC138; however, a follow-up, randomized, double-blind, phase III trial failed to demonstrate improved survival139. Concern over toxicity risks with nonsteroidal anti-inflammatory drugs (NSAIDs), which include COX2 inhibitors, has limited their utility140. Recently, a large randomized trial of canakinumab, an antibody targeting IL-1β in patients with atherosclerosis, showed that patients receiving canakinumab had a statistically significant reduction in new lung cancer incidence and mortality141. A phase III trial to evaluate the efficacy and safety of canakinumab as adjuvant therapy in patients with NSCLC is underway142 (Supplementary Table 1).
Immunotherapies
Immunotherapy aims to either improve immune cell function or inhibit immunosuppressive activity143. Inhibition of immunosuppressive signalling networks with ICI, which restores T cell-mediated antitumour immunity, has changed practice guidelines in multiple solid tumours including lung cancer. In 2015, nivolumab, a PD1 antibody targeting the PD1–PDL1 axis, became the first immune checkpoint inhibitor to be approved for treatment of NSCLC. Since then, other immune checkpoint inhibitors have been granted approval as either monotherapy or in combination with other agents (Supplementary Table 1). In the following subsections, we discuss the seminal trials that led to such approvals, as well as the current thinking on biomarkers predictive of response or resistance to ICI.
ICI monotherapy for metastatic NSCLC
There are currently three PD1 and PDL1 antibodies approved for the treatment of metastatic NSCLC in the second or third line. The approval of the PD1 antibody nivolumab was based on the results of two phase III trials — CheckMate 017, which enrolled patients with tumours with squamous histology, and CheckMate 057, which enrolled patients with tumours with non-squamous histology. In these studies, patients with advanced NSCLC who had progressed during or after prior therapy were randomly allocated nivolumab or docetaxel, a standard second-line chemotherapeutic agent. In both trials, the primary end point of OS was superior with nivolumab treatment144,145. A 3-year follow-up report from both trials showed that both OS and PFS significantly favoured nivolumab (OS: 17% versus 8%; PFS: 10% versus < 1%)146.
Subsequently, another PD1 antibody, pembrolizumab, was approved for previously treated patients with NSCLC (regardless of histology) whose tumours expressed PDL1 by immunohistochemistry. Initial approval was based on results from the large multicohort phase Ib KEYNOTE-001 trial, where pembrolizumab was used for the treatment of patients with metastatic NSCLC, some of whom had received prior therapy147. Subsequently, the KEYNOTE-010 study showed that pembrolizumab exhibited superior OS compared with docetaxel in patients with previously treated metastatic NSCLC whose tumours had at least 1% total PDL1 expression148. KEYNOTE-001 also found that response rates and survival were highest in patients expressing PDL1 in at least 50% of tumour cells. This finding was corroborated in a landmark phase III trial (KEYNOTE-024), where patients with untreated, metastatic NSCLC with tumours expressing PDL1 in ≥ 50% of cancer cells and with no activating EGFR or ALK mutations were randomized to receive pembrolizumab or standard platinum-doublet chemotherapy. In this study, OS, PFS and response rates were all significantly higher with pembrolizumab149. As a result, pembrolizumab alone without chemotherapy has become a current standard of care for this patient population.
Atezolizumab is currently the only PDL1 antibody approved for patients with previously treated metastatic NSCLC. Similar to the PD1 trials described above, the OAK trial showed superior survival with atezolizumab over docetaxel. This outcome was observed regardless of PDL1 expression levels on tumour cells or tumour-infiltrating immune cells150. Trials are in progress to evaluate the efficacy of other PDL1 antibodies, such as durvalumab and avelumab for the treatment of metastatic NSCLC. However, durvalumab has also been evaluated in patients with inoperable, locally advanced, non-metastatic (stage III) NSCLC in a randomized trial151. In this study, patients completing the standard treatment of combined chemotherapy and radiation were assigned to receive either durvalumab or placebo for 12 months. Remarkably, median PFS was threefold higher, and time to recurrence or death was nearly doubled with durvalumab. Furthermore, improvement was observed in both smokers and never smokers and at all levels of PDL1 expression in tumour cells. This has led to a rapid breakthrough designation by the FDA of durvalumab for locally advanced, stage III NSCLC with no progression after chemoradiation.
Collectively, ICI trials are rapidly changing the treatment landscape of patients with metastatic and locally advanced NSCLC. Importantly, second-line immunotherapy is becoming a standard for patients who have progressed on first-line chemotherapy alone using Eastern Cooperative Oncology Group (ECOG) performance status. In addition, while the approval of the PD1 antibody pembrolizumab for first-line therapy in patients with advanced NSCLC with tumours expressing PDL1 in ≥ 50% of cancer cells is revolutionary, only 25–50% of all patients with NSCLC express PDL1, with less than half of these expressing PDL1 at the regulatory mandated level of expression152. Further improvements in clinical outcomes require exploring the efficacy of various combination therapeutic strategies.
Combination therapy
To increase the response rates of current immunotherapies, a major focus is to find appropriate combinations to act synergistically to mount potent immunological responses153,154,155. Cytotoxic therapy such as chemotherapy and radiation may alter the TME to increase the efficacy of ICI. For example, cisplatin, some anthracyclines and radiation can induce immunogenic cell death, which increases tumour antigen load and increases MHC expression and antigen cross-presentation by activated DCs, leading to an influx of TILs2,153. On the basis of evidence from preclinical studies, the landmark trial KEYNOTE-189 randomized untreated patients with advanced non-squamous NSCLC regardless of PDL1 expression to standard chemotherapy plus pembrolizumab or standard chemotherapy alone156. All clinical outcome end points such as response rates, PFS and OS were higher with the combined therapy across all levels of PDL1 expression, including tumours with < 1% PDL1 expression. Another strategy currently being tested is the combination of two immune checkpoint inhibitors that target non-redundant pathways of T cell inactivation. The combination of the CTLA4 antibody ipilimumab and the PD1 antibody nivolumab showed promise in a phase I trial157. A larger phase III multipart trial (CheckMate 227) included a study randomizing patients with untreated, metastatic tumours with some level of PDL1 expression to nivolumab alone, nivolumab plus ipilimumab or standard chemotherapy158. There were two co-primary end points: PFS in all patients and PFS in patients with non-synonymous high tumour mutational burden (TMB) defined as ten or more mutations per megabase. PFS in all patients at 1 year was significantly higher with the combination of nivolumab and ipilimumab than with chemotherapy (31% versus 17%). Of the 44% of patients with high TMB, 1-year PFS with the ICI combination was 42% compared with 13% with chemotherapy alone and 29% with nivolumab monotherapy; yet, no significant difference between the treatment regimens in patients with low TMB was observed. Although this trial has not yet resulted in FDA approval for dual ICI therapy, it is notable for being the first trial to assess the value of TMB as an efficacious predictive biomarker when used as a predefined end point in a randomized lung cancer trial.
Other combination strategies are being explored in ongoing early-phase or more advanced clinical trials. These strategies include combining immune checkpoint inhibitors with epigenetic modifiers, oncolytic viruses or VEGF antibodies. The combination of atezolizumab with bevacizumab plus platinum-doublet chemotherapy has already been shown to elicit a survival advantage over chemotherapy plus bevacizumab alone159.
Given the successes above, the potential for other agents to synergize with ICI is being investigated in preclinical models. For example, extensive preclinical data suggest that radiation may not only contribute to local tumour control but may also augment a systemic antitumour immune response, a phenomenon known as the abscopal effect160. Radiation administered to a liver lesion in combination with anti-CTLA4 therapy improved metastatic disease in other organs in a patient with NSCLC161. However, several factors including the fractionation schedule, dosing, sequence, timing and safety need optimization. There is also increasing evidence suggesting that epigenetic drugs may improve the therapeutic responses of ICI162. For example, a histone deacetylase 6 (HDAC6) inhibitor increased T cell activation and improved the function of APCs, whereas the bromodomain inhibitor JQ1 attenuated CD4+FOXP3+ Treg cells in peripheral blood and single cell suspensions generated from human NSCLCs. Notably, in vivo validation was demonstrated, as combined treatment reduced tumour growth and improved survival in spontaneous mutant KRAS and EGFR-driven mouse models of lung adenocarcinoma163. Consistent with these findings, patients with NSCLC first primed with the DNA methyltransferase inhibitor 5-azacytidine showed improved responses to PD1 or PDL1 therapy164.
Resistance to immunotherapies
Undoubtedly, the past 5 years have ushered in a transformation in our treatment paradigms for lung cancer. However, despite these advances, most patients with NSCLC either do not respond to ICI or develop resistance after initial response with subsequent disease progression. This has generated an unmet clinical need for biomarkers to identify patients who may benefit from immunotherapies (Box 1) and a better understanding of the mechanisms of tumour escape.
Tumour immune evasion eventually develops through a variety of pathways including the emergence of antigen loss variants, defects in antigen presentation (human leukocyte antigen (HLA) loss, downregulation of MHC expression and mutations in β2 microglobulin, a component of MHC I molecules), defects in IFNγ signalling and/or activation of alternative inhibitory pathways such as other immune checkpoints or IDO. A recent study also identified LKB1 alterations as the most prevalent genomic driver of primary resistance to PD1 inhibitors in KRAS-mutant lung adenocarcinoma165,166. A deeper understanding of the complexities of immune response and evasion will further enable the design of more effective and durable immunotherapy regimens. Consequently, we advocate for preoperative or window of opportunity trials in earlier stages of disease, where tissue and blood is obtained before and during treatment and after surgical resection of the tumour mass. For example, 45% of patients had a major pathological response in a recent trial of preoperative anti-PD1 inhibition in early-stage operable disease167. Access to human material obtained before, during and after treatment and at the time of relapse for translational studies will provide great insight into the evolution of an effective immune response.
Pre-metastatic niche targeting
The pathways driving the establishment of a pre-metastatic niche constitute potential therapeutic targets for the prevention and early treatment of metastases. In preclinical models, an inhibitor of ALOX5 (known as zileuton and used as an asthma inhibitor) reduced lung metastasis by decreasing leukotriene production in neutrophils; notably, neutrophil counts remained unaffected98. In addition, targeting the neutrophil proteases cathepsin G and neutrophil elastase with the small molecule inhibitor sivelestat decreased lung metastases100, suggesting potential for clinical translation. While these studies support therapeutic targeting of the pro-metastatic role of neutrophils in cancer, importantly, such approaches must be applied with caution, as neutrophils also exert anti-metastatic activity in other experimental mouse models168. Lysyl oxidase-neutralizing antibodies have shown efficacy in preclinical studies169, and efforts are underway to develop antibodies for use in humans. Several studies have proposed therapies that inhibit the recruitment of immune cells to the pre-metastatic niche, including CXCR2 targeting to decrease platelet-mediated granulocyte recruitment170. Similarly, blockade of CCL2–CC-chemokine receptor 2 (CCR2) signalling reduced metastasis by decreasing mobilization of monocytes95. However, paradoxically, discontinuation of CCL2 inhibition led to a larger release of monocytes into the blood as well as increased angiogenesis and cancer cell proliferation in the lungs, resulting in reduced survival of the mice171. Harnessing potential targets from metastasis-suppressive niches is also being considered for therapy. For example, a peptide of five amino acids in length derived from prosaposin with TSP1-inducing activity reduced metastases formation in the lungs114.
Challenges and future directions
Despite major advancements in basic and clinical research pertaining to the role of the TME in lung cancer, several key questions remain to be addressed to create effective treatment opportunities so that optimal clinical outcomes are achieved.
Improving standard therapies
Antiangiogenic therapies have produced some favourable outcomes despite key limitations pertaining to dose-limiting toxicities, emergence of primary or acquired resistance and the lack of reliable validated biomarkers to guide selection of patients with NSCLC172,173. Current studies have focused on combining antiangiogenic agents with therapies targeting the cancer cell. For example, the combination of bevacizumab with the EGFR inhibitor erlotinib received approval as first-line treatment for patients with EGFR-mutant NSCLC in Europe in 2016 and is now being tested in the United States174.
In the clinical space of immunotherapy, the challenge is to increase response rates in patients with NSCLC, and a major effort towards finding predictive biomarkers for patient selection and combination agents to increase treatment efficacy is underway.
For example, an important barrier constitutes the lack of biomarkers to assess early responses to immunotherapy, and recently, circulating free DNA was used to assess immunotherapy response in lung cancer175.
Following the success of ipilimumab in combination with nivolumab in patients with NSCLC with high TMB158, other modalities including radiation, chemotherapy and antiangiogenic therapies are being tested176,177.
Recently, the combination of the VEGFR2 inhibitor ramucirumab and pembrolizumab showed a disease control rate of 85% in a phase I trial of patients with advanced NSCLC178.
Considerable enthusiasm has developed for the use of ICI in early-stage and locally advanced cancer179,180. The timing is pertinent, as implementation of low-dose computed tomography (CT) screening programmes in populations at risk has already begun to increase the number of patients with NSCLC diagnosed at an early stage181.
While such trials carry the promise of improving systemic immunity against occult metastases, several substantial challenges in this approach exist including defining the optimal treatment schema and appropriate drug combinations, measuring treatment responses as determined by the evaluation of tumour volume or immune-related responses and quantifiable end points (PFS and OS) and, importantly, the selection of patients who are likely to benefit.
Another challenge with immune checkpoint inhibitors is their ability to activate host immune responses, causing undesired adverse effects. Recently, immune checkpoint antibodies conjugated to a matrix-binding peptide, when administered directly into tumours, showed maximal retention in the tumour ECM and generated effective antitumour responses with minimal adverse effects182.
Technological advancements
Technological barriers need to be overcome to unravel the TME landscape and the intricate network of signalling pathways, as they may lead to the identification of prognostic and diagnostic biomarkers and targets for therapy development.
Emerging studies have begun to interrogate the complex tumour–stroma crosstalk in preclinical models41, which has led to the development of the computational software CCCExplorer, which assesses cell–cell communication pathways from multicellular genomic data sets41.
Recently, an innovative approach unravelled TME transcriptomes in human lung tumours at single cell resolution183. Other technological advancements in multiplexed immunohistochemical staining, multiparametric flow cytometry, cytometry by time of flight (CyTOF) and single cell sequencing have also resolved TME features directly in clinical specimens10,36,184,185.
Regression-based deconvolution of bulk gene expression data is being used to quantify specific cellular compositions of human tumours to predict clinical outcomes and for biomarker discovery and therapeutic target identification186.
This approach has the potential to be developed into a clinical test, as it does not rely on a predetermined panel of markers and can determine cellular heterogeneity from limited amounts of fresh, frozen and fixed clinical specimens.
The emerging area of radiomics has the potential to directly utilize medical images (positron emission tomography (PET), magnetic resonance imaging (MRI) and CT) to better define tumour spatial complexity and heterogeneity187. In preclinical models, real-time intravital optical imaging is beginning to be used to visualize dynamic cellular interactions during tumour progression, specifically between disseminated cancer cells and immune cells188 (Supplementary Movie 1).
Although imaging of the intact lung presents challenges owing to local respiratory motion within the lungs, this has now been overcome by using a vacuum stabilized imaging window188,189.
In addition, whole lung organ imaging was used to estimate 3D TAM composition and their response to CSF1R blockade in a KRAS-mutant xenograft mouse model of lung cancer190.
Developing better lung cancer models
Genetically engineered mouse models (GEMMs) carrying activating mutations in EGFR or KRAS, or EML4–ALK translocations, continue to provide key mechanistic insights related to TME reprogramming and function191,192,193.
However, GEMMs are unresponsive to single-agent immune checkpoint inhibitors194,195, which has been attributed to a low mutational burden and reduced lymphocytic infiltration196,197,198.
Whether these GEMMs can be used to provide mechanistic insights into non-responsiveness to ICI remains to be determined. Recently, immunocompetent mutant KRAS orthotopic mouse models with mutational burdens comparable to non-smoking early-stage patients with NSCLC have shown responses to single-agent immune checkpoint inhibitors70,199.
There is also an increased interest in using patient-derived xenograft (PDX) models, as they recapitulate aspects of individual patient tumours and have been predictive of clinical outcomes and precision medicine strategies200,201.
However, as immunodeficient mice used for propagating human tumours have a deficiency of key adaptive immune cells, efforts are underway to ‘humanize’ these models by engineering in human immune effectors and engrafting human peripheral blood mononuclear cells202.
However, additional barriers continue to limit the use of PDX models, such as potential mouse-specific evolution of the human tumours203 and mouse H2 but not HLA-restricted T cell education in the mouse thymus204.
A major effort in the field is to develop ex vivo human cancer models that can address the contribution of the microenvironment to tumour progression as a function of time. Ex vivo human NSCLC explant models, which have the advantage of retaining the TME, are being explored to evaluate response to therapy205.
Recently, a human NSCLC model was engineered on a chip that mimics organ microenvironment-specific cancer growth, tumour dormancy and responses to therapy over time206.
The pre-metastatic niche in the clinic
The pre-metastatic niche has potential clinical utility to identify patients with breast cancer who are at an increased risk of metastasis at the time of diagnosis of the primary tumour.
However, studies so far describing the pre-metastatic niche have been mainly performed in mouse models.
The observation that MDSCs secrete S100A8 and S100A9 in the pre-metastatic niche was used to develop S100A9-specific single-photon emission computed tomography (SPECT) whole body imaging to visualize pre-metastatic lungs of a preclinical model of breast cancer metastasis207.
Similarly, high-affinity PET radiopharmaceutical targeting of the α4β1 integrin was used to identify the pre-metastatic niche208. The clinical relevance of such an approach in identifying patients with breast cancer who are at increased risk of metastasis is awaited.
Deconstructing the complexity of the cellular and molecular interactions in the pre-metastatic niche in the human lung has proved challenging owing to a dearth of clinical specimens; however, the forthcoming implementation of rapid autopsy programmes is likely to yield such specimens.
Moreover, determining how long the pre-metastatic niche remains primed following surgery in patients with cancer is important because lung metastasis may develop months or years after surgical resection of the primary tumour.
Future investigations are also likely to focus on determining similarities and differences between the reprogrammed TME associated with the primary lung carcinoma and the pre-metastatic niche, as this would allow development of therapies that can selectively target either the primary or the secondary tumours in the lung.
The TME in precision medicine
Currently, personalized medicine approaches are focused on the evolution of mutant cancer genes to assess therapeutic responses209, and the utility of the TME has remained largely unexplored.
The role of the TME in influencing the treatment responses of cancer cells suggests opportunities for rational, precise and individualized treatments210. Given that the TME landscape is continually changing as a function of tumour evolution and treatment responses, molecular and functional imaging has the potential to match treatment regimens to the specific landscape in individual patients211.
Recent studies have also begun to include the TME as a predictive biomarker to identify patients who may benefit from immunotherapies149,212. However, other parameters including engagement of additional immune checkpoints, deficient T cell priming and the inflammatory state of the tumour (cold versus hot tumours) are being considered to guide precision immunotherapy approaches. Indeed, recently, an immunogenomic analysis of >10,000 tumours including lung cancer identified 6 immune subtypes that are likely to impact future prognostic and therapeutic strategies213 (Box 1).
It is expected that such multiscale profiling approaches will lead to the generation of a patient-specific TME atlas, with prognostic and therapeutic implications. Recently, the generation of autologous tumour organoids cocultured with peripheral blood lymphocytes from patients with NSCLC has the potential to assess the sensitivity of tumour cells to T cell-mediated killing in individual patients214.
Conclusion
The complex microenvironment of the lung supports the development of both primary lung carcinomas and metastasis from extrapulmonary neoplasms and offers an untapped resource of targets for therapy development.
Mechanistic insights into the tumour-reprogrammed microenvironmental landscape in lung cancer together with the development of drugs that specifically inhibit the components of the landscape have ushered in a new era of cancer medicine.
Particularly, certain immunotherapies have performed exceptionally well compared with standard chemotherapy and have the potential to become the new standard of care in a subset of advanced patients with NSCLC.
Identifying predictive biomarkers to optimize the benefit of these therapies remains a clinical challenge. Although both PDL1 and TMB are being used as predictive biomarkers to select for patients for therapy, many patients will not qualify just based on these two markers, and there is a requirement to develop additional biomarkers to ensure that larger patient populations benefit.
The concept that one size fits all is now obsolete, and this has ushered in the era of precision medicine in lung cancer, which is currently focused on individual molecular testing and cancer genomic analysis to help guide physicians to identify appropriate therapies.
However, to maximize patient outcomes, the stage is set to combine the genetic information with the TME landscape, which may allow development of rationally designed combination therapies.
Importantly, the success of targeting angiogenesis and immune cells has reinvigorated enthusiasm in elucidating the prognostic and pathophysiological roles of other components of the TME in lung cancer to enable clinical evaluation.
For references, please click on the above link.