LIFE EXTENSION MAGAZINE
February 2017

By William Faloon

William Faloon
The prevalence of kidney disease is increasing in persons 60 years and older. This has led researchers to investigate what new factor is behind this mounting kidney failure problem.
To put this in perspective, a study period ending in 1994 found chronic kidney diseasepresent in 18.8% of older individuals. A study period ending in 2008 found chronic kidney disease in this same age group (60+ years) had surged to 26%. That’s a 38%increase over a time-frame of only 14 years.2
More than 1 in 10 American adults now have some stage of chronic kidney disease.1 Many are unaware of their kidneys failing and the increased risk for heart disease that this carries.3
Those afflicted with chronic kidney disease have higher homocysteine4,5 and C-reactive protein6,7 levels, along with reduced production of nitric oxide.8,9 So it is not surprising that kidney impairment elevates vascular disease risk.10
So why is kidney disease skyrocketing in persons over age 60?
Hypertension has long been a prime factor, but greater steps to control blood pressure have been taken in more recent years.
Diabetes is a culprit and poor glycemic control has been on the rise, as are increases in average body (fat) mass.
Overlooked is the impact that drugs have on the kidneys. Common pain relievers such as ibuprofen are notoriously damaging to kidneys, yet few warnings about their nephrotoxic effects are provided to consumers.11,12
The new report found risk of kidney damage is dose dependent. People who took two daily doses of drugs like Prilosec® or Prevacid® had a higher risk compared to one daily-dose users.
One aspect of the study analysis suggests twice-daily proton pump inhibitor dosing was associated with a 46%higher risk of chronic kidney disease than once-daily dosing, which was associated with a 15% higher risk.1
Fundamental changes to reverse this upward trend of kidney disease are urgently needed.
This article will make some suggestions about protecting renal function as we age, and what those who suffer gastroesophageal reflux (GERD) should change in light of the disturbing findings about proton pump inhibitors.
Heartburn (acid reflux) has plagued mankind throughout recorded history. Some of our founding fathers suffered horrific bouts of heartburn for which there was no effective treatment.13
In 1992, I woke up to a sharp stabbing pain in my chest. A quick visit to a gastroenterologist resulted in a diagnosis of esophagitis (caused by reflux). A proton pump inhibitor drug (Prilosec®) was prescribed and my pain disappeared in a few days.
What did people do before proton pump inhibitors were discovered I wondered? Unlike older medications (such as Tagamet®) that only reduce stomach acid, proton pump inhibitors block it altogether (if used every 12 hours).
Considering that up to 30% of Americans have symptomatic heartburn that occurs at least once weekly, and more than 40% of Americans have it to one degree or another,14 the advent of proton pump inhibitors would have been a miraculous solution—if it were not for the side effects that occur when stomach acid is chronically blocked.
Increased Fracture Risk in Users of Proton Pump Inhibitors

Proton pump inhibiting drugs block stomach acid production, which often provides rapid relief from heartburn symptoms. Yet hydrochloric acid secreted by our stomach is needed to break down foods to facilitate absorption of essential nutrients.
As people age, the gradual decline in stomach acid production makes it difficult to absorb minerals. Chronic use of proton pump inhibitor drugs can severely impair absorption of calcium, magnesium, iron and certain vitamins.15-19
Proton pump inhibitors are now considered to be culprits behind higher rates of osteoporosis.20,21 Studies show that regular users of proton pump inhibitors have a 10% to 40% increased risk of bone fractures.15,22-27
In addition, users of these heartburn-relieving drugs suffer higher incidences of pneumonia and bacterial infection (Clostridium difficile).28,29
Vitamin B12 Deficits
Stomach acid is part of the digestive juices needed to absorb vitamin B12. You need acid to separate vitamin B12 from food.
When stomach acid is blocked for an extended period, vitamin B12 deficiencies occur30-32 and can manifest as neurological impairment (sometimes leading to dementia),33 anemia,34 elevated homocysteine,35 and other disorders.
One study found that vitamin B12 deficiency was 65% more common in long-term users of proton pump inhibitors.32 The degree of the B12 deficit correlated with the dose of the proton pump inhibiting drug, i.e. the higher the daily dose, the greater the B12 deficit.
Discontinuation of the proton pump inhibitor resulted in a reversal of the vitamin B12 deficit.32
Those who need to take daily proton pump inhibitors can obtain sufficient B12 levels by taking 1,000 mcg injections of B12 three times a week, or by taking daily sublingual B12 lozenges.
Heart Attacks in Proton Pump Inhibitor Users

Stomach acid is required for optimal absorption of nutrients like selenium and magnesium. Aging individuals who don’t supplement with essential nutrients are often deficient. If they take a proton pump inhibitor and don’t supplement, they are at risk for severe nutrient deficiencies.
When the body is deprived of calcium, it robs it from the bones, which results in release of bony constituents that contribute to coronary artery calcification.36,37
The mineral deficit most frequently associated with proton pump inhibitor use is magnesium. Several studies show frank magnesium deficits in response to suppressing stomach acid with proton pump inhibitors.17,18,38
So it should come as no surprise that people who regularly use proton pump inhibitors suffer heart attack rates higher than nonusers.39-41 A recent study found a 1.58-fold greater risk of heart attack amongst proton pump inhibitor users.39
Users of acid-blocking drugs not only suffer magnesium deficiency, but a lack of vitamin B12 causes their homocysteine levels to surge. These twin vascular risk factors help explain the higher risk of heart attack and stroke in long-term proton pump inhibitor users.
Kidney Damage
Scientists grew suspicious of proton pump inhibitors because they can cause acute interstitial nephritis,42-44 a condition in which spaces between the kidney tubules become swollen and interfere with filtration of toxins out of one’s blood.45
A large case-control study published in 2013 revealed that patients presenting with acute kidney failure were more than twice as likely to be using a proton pump inhibitor drug.46 Typically, acute kidney-failure patients recover rapidly after they withdraw from proton pump inhibiting drugs, but it may take up to three months and in some cases require additional therapy.47
Based on data showing proton pump inhibitors create acute kidney problems, researchers at Johns Hopkins University sought to evaluate the impact on a large group of people over a 6-year period.
A total of 10,482 subjects with a mean age of 63 years were selected from a study titled Atherosclerosis Risk in Communities. The study used several forms of analysis to rule out confounding factors that might have caused chronic kidney disease. The findings from this study published in 2016 revealed that regular proton pump inhibitor use was associated with:1
- 35% increased incidence of chronic kidney disease (time-varying analysis)
- 45% increased incidence of chronic kidney disease (unadjusted analysis)
- 50% increased incidence of chronic kidney disease (adjusted analysis that took into account demographic, socioeconomic and clinical variables)
Proton pump inhibitor users were more likely obese and taking antihypertensive medications, which might have increased chronic kidney disease incidences beyond that associated with acid-blocker drugs like Nexium®, Prilosec®, and Prevacid®.
Interestingly, GERD patients who used older drugs like Tagamet® did not show an increase in chronic kidney disease incidence.
A large study published in 2016 confirmed these findings. The study’s authors compared users of proton pump inhibitors (Nexium®, Prevacid®, et al.) to older line drugs like Tagamet® (cimetidine). Patients who took the proton pump inhibitors had a 96% increased risk of developing kidney failure and a 28% increased risk of chronic kidney disease.48
Although we know that hypertension, heart disease, diabetes, and family history are risk factors for kidney disease,49 these findings suggest that proton pump inhibitors are also associated with chronic kidney disease and kidney failure afflicting older individuals.
What GERD Sufferers Should Do

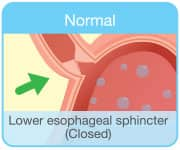
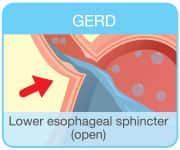
GERD can be a frustrating, vexing problem. It is not caused by excess stomach acid.
The underlying reason for GERD is failure of the sphincter valve between the stomach and esophagus to properly close. This enables stomach contents that include enzymes, food, drink, bile, and acids to reflux back up into the delicate esophageal lining. The outward symptomatic effect is heartburn. The long term impact can be an increased risk for Barrett’s esophagus, a type of change in the epithelium (lining) of the esophagus which may increase the risk for a type of esophageal cancer.50-52 Though the increase in risk of Barrett’s esophagus is not known with certainty, most medical experts suggest the long-term risk is around 15%-20%, which necessitates an upper endoscopy to assess the esophagus lining every three to five years in chronic GERD sufferers.53-55
Lifestyle modifications that can mitigate or eliminate GERD include weight loss, reducing or eliminating caffeine/alcohol/nicotine, reducing meal size, not eating late in the evening, and elevating the head end of one’s bed so that gravity holds down stomach contents that otherwise enter the esophagus while one sleeps.56-61
While these GERD-mitigating steps work reasonably well, few people implement them consistently.
The convenience of taking a proton pump inhibitor to prevent heartburn has resulted in large swaths of the aging population taking this drug every day, but doing nothing to correct the underlying problem causing GERD.
QUOTE FROM STUDY PUBLISHED BY AMERICAN MEDICAL ASSOCIATION
“Chronic kidney disease (CKD) affects approximately 13.6% of adults in the United States, is associated with a substantially increased risk of death and cardiovascular events, and accounts for a disproportionately large burden on the financial resources of Medicare. The increasing prevalence of CKD among communities cannot be fully explained by trends in known risk factors, such as diabetes mellitus and hypertension, suggesting that other variables may contribute to the disease process. Medication use may be a potential factor, particularly given tendencies toward polypharmacy. Identifying iatrogenic risk factors for CKD may help to promote the rational use of medications and reduce the burden of CKD worldwide.”1
“Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease,” JAMA Internal Medicine,February, 2016.
Raft-Forming Alginates
Several years ago, Life Extension® introduced a chewable tablet that, when taken during a meal, forms a temporary protective barrier between the stomach and esophagus to prevent stomach contents from refluxing.
Most users found the chewing of these tablets at mealtime to be inconvenient and did not continue with them. This is somewhat understandable considering how easy it is to pop a 20 mg tablet of Prilosec® (omeprazole) once or twice a day to stop heartburn symptoms from manifesting.
With data mounting about the side effects of long-term use of proton pump inhibitors, those with mild to moderate GERD should consider lifestyle changes and a new approach described in this issue of Life Extension.
Severe GERD sufferers should strike a balance between a less frequent dose of the proton pump inhibitor, once symptoms are resolved, and “on demand” therapy if appropriate.
Lifestyle modifications and occasional use of raft-forming alginates should be considered to give the body a break from chronic proton pump inhibitor use.
Sublingual and/or vitamin B12 injections are recommended for those who continue daily use of proton pump inhibitors (hopefully no more than once a day).
New Chewable Antacid Tablets
The article on page 40 of this issue describes a novel antacid utilizing magnesium, calcium, and licorice extract. This unique formula is designed to neutralize acid in the esophagus and promote movement of stomach contents away from the delicate esophageal lining.
This antacid lozenge can help GERD sufferers reduce or eliminate reliance on proton pump inhibitor drugs.
OUR FRAGILE KIDNEYS
 |
Most people don’t understand the delicate nature of the tiny structures that comprise their kidneys. Even fewer realize that kidney function involves more than merely removing toxic waste from the blood.
The kidneys support water/fluid balance, secrete hormones to make red blood cells, maintain electrolyte levels and regulate blood pressure. They are also involved in maintaining healthier levels of precursors to endothelial nitric oxide.
Every day, our two kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine.62
Those with chronic kidney disease often have sharply higher homocysteine and C-reactive protein levels that predispose them to a myriad of cardiovascular disorders.
Maintaining youthful kidney function is of utmost importance if one’s goal is to live a long and healthy life. Yet far too little attention is paid to these critical organs. Documented chronic kidney disease risk factors are:
- Diabetes63-65 and metabolic syndrome66
- High blood pressure64,67
- Obesity64,68
- Toxic medications69,70
Overlooked is the adverse impact that poor dietary patterns and normal aging inflict on the fragile structures (glomeruli) that comprise the filtering units of our kidneys.
Supplemental nutrients that have been shown to protect and support healthy kidney function include coenzyme Q10,71,72 omega-3s oils,73,74 and N-acetylcysteine.75,76
Importance of Blood Tests to Evaluate Kidney Health

No one should wait for kidney disease to manifest where it may progress toward end-stage renal failure. This is especially important for users of proton pump inhibitors (and pain relieving drugs).
A comprehensive CBC/chemistry blood test evaluates markers of kidney function such as creatinine and blood urea nitrogen.
The safe upper limit for serum creatinine is 1.00 (mg/dL). Any fractional number over this (such as 1.1) raises concern that can signal the need for the most accurate blood test to evaluate kidney function, called cystatin-C.
Cystatin-C is an underutilized blood marker, which is regrettable because it provides a far more accurate indicator of kidney function than the standard kidney tests.77 Optimal levels of cystatin-C are less than 0.91 mg/L. Any result that comes back higher indicates the presence of kidney disease.
If caught in time, cystatin-C levels can be brought back to normal by discontinuing suspected drugs, such as ibuprofen and/or a proton pump inhibitor.
The only factor that impedes routine use of the cystatin-C blood test is its high cost. Commercial labs charge around $200 for it. Life Extension offers the cystatin-C blood test to consumers for $99.
A comprehensive CBC/chemistry blood test that includes dozens of important markers such as glucose, lipids, and blood counts, along with markers of liver and kidney function, can be obtained directly from Life Extension for only $35.
Cystatin-C provides an earlier indicator of kidney impairment than tests like creatinine that are included in the CBC/chemistry panel.
In light of the new findings, long-term users of proton pump inhibitors should consider ordering the cystatin-Cblood test as this provides the earliest warning to cut back or discontinue use of proton pump inhibitor drugs. The CBC/chemistry and/or cystatin-C blood tests can be ordered by calling 1-800-208-3444 or at LifeExtension.com/CBCPlus
Try Reducing Frequency and Dose – “On Demand” Therapy
A number of published papers conclude that Americans are overusing proton pump inhibitor drugs.78-80
The medical literature reveals a dose-response relationship regarding the side effects these drugs induce.1
As reported in the introduction to this article, a recent study has observed increased risks of chronic kidney disease in users of proton pump inhibitors, and the risk may be higher in those who take two doses a day instead of one. Most proton pump inhibitors start to wear off after 12 hours, so by taking only one of these drugs a day, there is at least some restoration of stomach acid production to help better absorb vital nutrients.
Studies dating back 25 years, however, demonstrate that proton pump inhibitors themselves can induce acute interstitial nephritis, which is a condition in which spaces between the kidney tubules become swollen and interfere with filtration of toxins out of one’s blood.81-83
These data should prompt you to consider reducing the dose frequency of your proton pump inhibitor medication to three times per week. Studies that have examined the possibility of intermittent therapy in patients with GERD, however, have been inconsistent as it relates to heartburn relief.
All things considered, an attempt to restrict intake of proton pump inhibitors to “on-demand” dosing, along with the regular use of a novel antacid lozenge described in this issue, may be an effective alternative solution to chronic use of acid-suppressing drugs.
Don’t Be a Victim of Medical Ignorance

Proton pump inhibitor drugs provide almost immediate relief from heartburn symptoms and can facilitate a cure for esophagitis.
In 2013, more than 15 million Americans were prescribed proton pump inhibitors and many more bought this class of drug over the counter.1,84 Study findings suggest that chronic prescribing of these drugs is not medically indicated in many cases.85 One study found that 27% of long term proton pump inhibitor users could discontinue therapy without encountering symptoms.86
Published studies show consistent associations between use of these acid-blocking drugs and higher risk of chronic kidney disease.42,43,46,48 This disorder has increased in prevalence during a time period that corresponds with widespread use of proton pump inhibitors.1,48
Many GERD sufferers have come to rely on proton pump inhibitors to offset the heartburn-inducing effects of eating large meals, excessive ethanol consumption and carrying too much weight.
Common-sense lifestyle changes can enable those with GERD to reduce or eliminate reliance on proton pump inhibitors.
A preponderance of clinical data indicates that this will beneficially result in a reduction in risks of bone fracture, heart attack, stroke, infections, dementia, and kidney failure.
Blood tests can readily reveal if kidney damage is occurring and provide an early warning to discontinue certain drugs before permanent kidney damage manifests.
Please turn this page to see how easy it is to obtain low-cost blood tests that can help you maintain optimalhealth throughout the New Year.
For longer life,
William Faloon